2025

Diagnosis is one of the most challenging and complex tasks faced by clinicians, and excellence in the diagnostic process involves both the art and science of medicine.

Monash University's 1 day Symposium on Improving Diagnosis was held on December 15 2025 with the theme “The Art and Science of Diagnosis”.
Date: Monday 15 December 2025
Time: 8.30am - 5.00pm
Venue: Learning and Teaching Building, Room G31, 19 Ancora Imparo Way, Clayton Campus
-
Keynote presentations

Event details
Diagnostic excellence resources
View

Symposium convenors and speakers were each invited to submit a couple of resources to share with attendees. The resources are collected here and include a mix of speakers' work, material relevant to symposium topics, and other items that might be of interest to symposium attendees.
-
-
The Community Improving Diagnosis in Medicine - CDIM
Read more
-
Demystifying cognitive bias in the diagnostic process for frontline clinicians and educators; new words for old ideas
Read more
-
Enabling diagnostic excellence in the real world: Managing complexity, uncertainty and clinical responsibility
Read more
-
Supplementary material 1 and 2
Download PDF
-
The Idiom’s Guide to Cognitive Bias in Diagnosis
Download PDF
-
A systematic review and meta-analysis of diagnostic performance comparison between generative AI and physicians
Download PDF
-
Using conversant artificial intelligence to improve diagnostic reasoning: ready for prime time?
Download PDF
-
Understanding and Communicating Uncertainty in Achieving Diagnostic Excellence
Read more
-
‘More than words’ – Interpersonal communication, cognitive bias and diagnostic errors
Read more
-
Communication of Diagnostic Uncertainty in Primary Care and Its Impact on Patient Experience: an Integrative Systematic Review
Read more
-
Cognitive Dissonance: How Self-Protective Distortions Can Undermine Clinical Judgment
Read more
-
Remember That Patient You Saw…’: Advice for Trainees on Coping After Making an Error
Read more
-
A growth mindset approach to preparing trainees for medical error
Read more
-
Looking with Uncertainty with Alexa Miller
Listen to podcast
-
Curiosity by Faith Fitzgerald
Read more
-
Varieties of uncertainty in health care: a conceptual taxonomy
Read more
-
An organisational approach to improving diagnostic safety
Download PDF
-
Diagnostic error: incidence, impacts, causes and preventive strategies
Download PDF
Keynote speakers
View
Oral abstracts
View
Session 3A (Room 2.21) | |||
3.A.1 Diagnostic Errors: Understanding Healthcare Practitioners’ Medico-Legal LiabilityDr Pamela J. Ferrada, Member Education, Knowledge and Research Manager, Risk Education, Medical Indemnity Protection Society Background & Aims: This presentation aims to establish a foundational understanding of some of the legal aspects of health practitioner liability arising from diagnostic errors. Key concepts in medical negligence laws, and professional duties related to anticipating, preventing and mitigating medicolegal risks will be discussed. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:Healthcare practitioners have a legal duty of care to provide a reasonable standard of care. Misdiagnosis, delayed or failure to diagnose may constitute a breach of this duty, leading to potential claims or complaints. Understanding the legal principles of medical negligence frameworks may assist clinicians in mitigating risks and improving patient safety. | |||
3.A.2 Could it be HIV Increasing HIV Testing in Clinical Indicator Settings?Louise Owen, Statewide Sexual Health Service, Tasmania, School of Medicine, University of Tasmania Key words (max 5): Background & Aims: Many people with delayed HIV diagnosis have often interacted with different healthcare services in the years before their diagnosis. Often, they have presented with clinical indicators that should prompt healthcare professionals to test for HIV, even if they do not fit the typical risk profile. We must increase proactive HIV testing within clinical settings and empower healthcare professionals to offer these individuals a HIV test. By proactively recognising these indicators and testing for HIV, any positive cases, previously undiagnosed, can receive prompt medical intervention to improve medical outcomes and impact HIV transmission, or HIV can be ruled out. Methodology, Approach, Innovation or Intervention:Integrating HIV testing into standard clinical practice for all patients presenting with potential signs and symptoms of HIV, regardless of their sexual orientation or number of sexual partners, will help normalise HIV testing and decrease stigma and fear. This approach can lead to earlier diagnosis and better health outcomes for individuals living with HIV. Testing for HIV also remains cost-effective, even when the initial likelihood of a positive result is as low as 1 in 1,000 cases, Raising awareness to broad groups of clinicians, including at college level to enact change in guidelines to normalise HIV testing will help achieve the goal of zero HIV transmissions in Aust by 2030. There are a number of great resources for clinicians ASHM
Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:Normalise HIV testing in multiple clinical situations and empower clinicians to feel comfortable to test, rule out HIV and ensure this cheap, sensitive and specific test is used early on in the diagnostic cascade for many clinical indicator conditions;
| |||
3.A.3 Exploration of in-hospital code stroke activationNadja Korajkic, Lauren Sanders - Department of Neurosciences, St Vincent’s Hospital, Melbourne, VIC, Australia Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Data were evaluated against recommended stroke key performance indicators, as well as exploration for common factors associated with stroke code activation Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:Inpatients under some units are at a higher risk of experiencing inpatient stroke with requirement for acute stroke treatment. Exploring interventions to identify and minimise this risk may be of benefit. | |||
3.A.4 The Outpatient Emergency Department Pathway to Cancer Diagnosis: Healthcare Engagement and Rural Treatment DisparitiesCaroline Thompson, University of North Carolina at Chapel Hill Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:The outpatient ED pathway affects engaged patients across healthcare settings, representing coordination failure rather than patient disengagement. Rural patients face compounding vulnerabilities: higher pathway prevalence despite similar engagement, and subsequent treatment barriers particularly for surgical oncology. | |||
3.A.5 Absent Initial Clinical Impressions in ED: Time to Get Back to BasicsProf Diana Egerton-Warburton*1,3, A/Prof Lisa Kuhn 3,4, Joanne Enticott 2,3, Suzanne Bumpstead 1,3, Dr Neil Goldie 3, Dr Helen Pshiogios 3 et al. Affiliations 1. Monash University, School of Clinical Science at Monash Health, Key words (max 5): Background & Aims: This study aims to assess the adequacy of the initial clinical impression and management plans documented in EMR for adult patients presenting to EDs. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Almost one-quarter of adult ED patients lacked a documented clinical impression in their initial medical assessment, irrespective of clinician experience and the four most urgent triage categories. This gap should be addressed rapidly to improve diagnostic decision-making and optimise patient safety. Educational impact, Further development or Future applications: Lessons learnt/take-home messages: The absence of clinical impressions should be addressed rapidly to improve diagnostic decision-making and optimise patient safety. | |||
3.A.6 Implementation of a structured clinical impression and management dotphrase in the electronic medical record as standard practice at Monash Health Emergency Departments: A stepped-wedge cluster-controlled analysis of the impactProf Diana Egerton-Warburton*1,3, Joanne Enticott 2,3, Parneet Sethi 2,3, Suzanne Bumpstead 1,3, Sophie Balzat 3, Veena Peacock 3 et al. Affiliations 1. Monash University, School of Clinical Science at Monash Health, Key words (max 5): Background & Aims: This study aims to measure the impact of the introduction of a co-designed EMR Nudge (‘DotPhrase’) for clinical impression and management in initial assessments in Emergency Departments (ED) patients. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:DotPhrase use is associated with improved documentation of clinical impressions, differential diagnosis and cross-checking. The DotPhrase shows promise in its role as a clinical decision-making adjunct. Monitoring and providing feedback to staff regarding the use of the EMR ‘DotPhrase’ together with ongoing education regarding the importance of documenting a clinical impression and management plan in the ED Initial Assessment, is essential to ensure sustainable change. |
Session 3B (Room 2.31) | |||
3.B.1 Humanities in Monash Medicine - A Visual Arts Program to Enhance SkillsDeborah Leach, Monash Medical School Key words (max 5): Background & Aims: Humanities based teaching in medicine is acknowledged to be an effective method to develop core clinical skills underpinning diagnostic excellence. It provides an opportunity for re-conceptualising the ways in which we teach students to observe, listen, work with others and reflect on their attitudes and cognition. Methodology, Approach, Innovation or Intervention: Sessions using an array of curated activities such as Personal response Tour (PRT) and Visual Thinking Strategies (VTS) were offered at strategic points in the medicine course including major transition points, curriculum with challenging topics and sessions specifically designed to support professionalism development in students. Most sessions were run in the National Gallery of Victoria but sessions were also successfully run in campus based classrooms using a transportable collection of gallery images. This program intentionally complements the current curriculum through the course which includes mindfulness teaching (pre-clinical), Healer's Art (Year 3B) and compassion training (final year). Not only do students benefit from skills acquisition, but the inclusion of humanities also injects joy into learning. Discussion, Outcomes or Findings: Specific comments about what students had learned related to important aspects of clinical thinking, not leaping to conclusions and careful listening to members of the care team. Many students reflected on the importance of observing and listening to understand both team and patient perspectives so that the goals for each patient are achieved. Educational impact, Further development or Future applications: In 2026 Art of Seeing will be expanded to provide Indigenous Health teaching to metropolitan final year students in addition to the other activities offered in 2025. Development of faculty to help design and facilitate sessions will be critical to the success and sustainability of the program. Lessons learnt/take-home messages:Introducing a program that is very different from usual university teaching methods requires time, patience, careful integration and a view to creating sustainability. | |||
3.B.2 Designing a Decision-Making Flowchart to Reduce Unnecessary CXR Ordering in the Emergency DepartmentDereck Luk, Joseph Miller, Bronwyn Kirkwood, Elizabeth Cole, Rae-lee Wilkinson, Sarah Zheng, Raewyn Szelag, Shaun Eccles-Smith, Ilya Kardailsky, Erin Woodward, Paul Roche, Paul Buntine Key words (max 5): Background & Aims: Our aims are as follows: 1. To evaluate the difference in diagnostic yield between CXRs ordered after clinicians viewed the flowchart compared to those ordered by clinicians not following the flowchart. 2. To compare the yield of positive findings between patients seen by a doctor and those unseen at the time of CXR ordering. 3. To assess the rate and nature of incidental findings (i.e. abnormalities not related to the presenting complaint) that require follow-up. Ultimately, the goal is to reduce inappropriate CXR orders while maintaining diagnostic safety. Methodology, Approach, Innovation or Intervention: Data collection includes patient details, initial presenting complaints, CXR indication, CXR report findings, diagnosis, and final treatment or management outcomes. Findings will be classified as follows:
Approximately 60–100 cases will be reviewed under the new flowchart. Comparisons will be made between flowchart-adherent and non-adherent cases, as well as between patients who have and have not been seen face-to-face by a clinician. Discussion, Outcomes or Findings: These early findings form the foundation of our expected outcomes, suggesting that adherence to the flowchart improves diagnostic yield while premature ordering does not improve diagnostic yield. The current sample size is too small to permit statistical significance testing, but we will continue with data collection with the goal of highlighting opportunities to improve diagnostic efficiency and reduce low-value imaging. Educational impact, Further development or Future applications: Lessons learnt/take-home messages: | |||
3.B.3 Developing Diagnostic Competencies for Nurse-led Pathways in the Emergency DepartmentDeborah Digman Royal Victorian Eye and Ear Hospital, Melbourne Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Nurses first completed a competency in the use of the slit lamp to ensure their foundational diagnostic skills were sound. Following this they progressed to completing diagnostic competencies in the above fast track conditions, with case by case oversight by consultant ophthalmologists. Discussion, Outcomes or Findings: Consultant ophthalmologists or senior eye registrars will continue to work closely with the nursing staff, even once a competency has been achieved, modelling ongoing diagnostic cross- checking and team- based diagnosis. Educational impact, Further development or Future applications: Lessons learnt/take-home messages: Team-based diagnosis requires medical and nursing clinicians and educators to work closely together. In this project, this included working together both in the development of nursing diagnostic competencies and in the application of these competencies on the ED floor to ensure diagnostic excellence. | |||
3.B.4 Investigation FrameworkBirks J, Birks R, Seach K, Haigh C Monash Rural Health Gippsland Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:This pilot study of an Investigation Framework to structure the learning of clinical reasoning for medical students has been well received. Students appreciate guidance as they navigate the overwhelming number of options when requesting investigations. | |||
3.B.5 Learning to Diagnose: Leveraging cognitive load theory (CLT) and metacognition to reduce diagnostic errorsDr Pamela J. Ferrada, Member Education, Knowledge and Research Manager, Medical Indemnity Protection Society Key words (max 5): Background & Aims: This presentation aims to establish explicit connections between CLT, metacognition, and their practical application in clinical work, particularly in relation to minimising the risk of missed or delayed diagnosis. Key concepts related to cognitive load types (extraneous, intrinsic and germane) will be discussed and their relevance in the content of minimising diagnostic errors. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages: | |||
3.B.6 Evaluation of the Diagnostic Yield of CT and MR Modalities in Clinical Indications of Cranial Nerve PalsiesAaron Avenido, Melbourne Medical School, The University of Melbourne A/Prof Jean Lee, Department of Public Imaging Services, St Vincent's Hospital Melbourne Key words (max 5): Background & Aims: Although CT angiography is now the modality of choice for emergent neuroimaging of oculomotor nerve palsies, due to its speed and high sensitivity for aneurysms, there is limited consensus regarding the benefit of CT and MR neuroimaging in other palsies. Namely, whether clinically useful intracranial causes can be found. In fact, MR is traditionally contraindicated in those aged over 50 years old, due to the lower epidemiological likelihood of detecting non-aneurysmal pathologies. Consequently, this study aims to investigate and compare the diagnostic yield of CT and MR modalities in clinically suspected and diagnosed cases of cranial nerve palsies at St Vincent's Hospital Melbourne. This is a major metropolitan tertiary centre with a sufficient case load of ocular palsies. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages: |
Session 3C (Room 2.37) | |||
3.C.1 A Worried Parent is the Most Vital SignErin Mills (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED), Phyllis Lin (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED), Mohammad Asghari-Jafarabadi (Monash Uni/School of Public Health and Preventative Medicine, Monash University/Department of Clinical Sciences/Department of Psychiatry, Monash Health/Paediatric ED), Adam West (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED), Simon Craig (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED) Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:A parent or carer expressing concern about clinical deterioration in their child is more strongly associated with critical illness in that child than any abnormal vital sign. The authors advocate that the concerns of parents or carers should be proactively sought by staff as part of routine clinical care. | |||
3.C.2 The Relationship Between Patient or Caregiver Concern for Clinical Deterioration and Critical Illness in an Adult Population - A Retrospective Observational Cohort StudyTom Truscott (Monash University/School of Clinical Sciences), Erin Mills (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED), Phyllis Lin (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED), Simon Craig (Monash Uni/School of Clin Sciences/Dept of Paediatrics, Monash Health/Paediatric ED) Key words (max 5): Background & Aims: The aims of this work were: - to determine the relationship between patient or caregiver concern for deterioration and critical illness in an adult hospital population, and - to compare the association between patient or caregiver concern for clinical deterioration and critical illness with the association between abnormal vital signs and critical illness. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages: *note this is a follow-on to our work in paediatrics (abstract titled "A worried parent is the most vital sign"), and follows very similar methodology. Happy to present one or the other, a talk combining the two, or back-to-back presentations* | |||
3.C.3 How Creating a Safe Space for Patients Leads to Greater Diagnostic AccuracyA/Prof Jennifer Neil, Monash Medical School, Monash University Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages:TVIC is a universal approach that recognises that any patients may have a history of abuse and violence. Patients with a history of abuse and violence commonly present to their health professional with physical, mental and reproductive issues. Through both organisational and individual approaches, a TVIC approach creates a safe space for patients to disclose their experiences of abuse and violence which not only brings diagnostic clarity but also allows patients to start the process of healing both physically and psychologically. | |||
3.C.4 Communicating Difficult Diagnoses in the Emergency DepartmentGifar Hassan, RVEEH Key words (max 5): Background & Aims: Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: In our department these difficult diagnoses include brain tumours, multiple sclerosis, giant cell arteritis, cerebral aneurysms and stroke. As clinicians in the ED, our role is to assess and initiate urgent treatments. We are often in the position where a patient wants more clarity regarding diagnosis and prognosis, however we can find ourselves unable to provide these answers. My talk will discuss these challenges and how we can improve patient- clinician communication and the patient experience. Educational impact, Further development or Future applications: Lessons learnt/take-home messages:Discussion of difficult and life changing diagnoses with patients requires preparation and training to improve the patient experience. | |||
3.C.5 Let‘s talk about HIV – Showcasing an Educational Partnership with People Living with HIV and Health Care Workers to Address Diagnostic StigmaJen Johnson, Living Positive Victoria; Richard Keane (presenting), Living Positive Victoria; Elizabeth Crock, Bolton Clarke. Key words (max 5): Background & Aims: Stigma remains the greatest barrier to care with healthcare settings being common sites of discrimination and privacy breaches. There are no brief video interventions specifically targeting this workforce. Methodology, Approach, Innovation or Intervention: Discussion, Outcomes or Findings: Educational impact, Further development or Future applications: Lessons learnt/take-home messages: | |||
3.C.6 The Art of Transforming Patient Feedback About Diagnostic Error into Diagnostic ExcellenceCarmel Crock, Royal Victorian Eye and Ear Hospital Key words (max 5): Background & Aims: In this study we sought to collate and analyse feedback from patients relating to diagnostic safety events in a busy emergency department. Methodology, Approach, Innovation or Intervention: We examined incidents entered into the system from the emergency department in the last 12 months and identified those relating to delayed, wrong or missed diagnoses. Themes of the patient feedback will be discussed from both the written feedback and oral feedback later solicited from the patient. Themes from a smaller number of diagnostic safety incidents reported by family members and carers will also be discussed. Discussion, Outcomes or Findings: Listening to feedback from patients in the advent of a diagnostic error is crucial to understanding contributing factors, learning from error as well as contributing to the healing process for patients and rebuilding trust. Ideally healthcare organisations would routinely collect patient feedback on diagnosis as part of the patient experience. Proposed methods for systematically gathering patient feedback to enhance the diagnostic process will be discussed. Such measures would ensure meaningful patient engagement in the diagnostic process, leading to a culture of continuous improvement in diagnosis and diagnostic excellence. Educational impact, Further development or Future applications: Lessons learnt/take-home messages:For patients to be fully engaged in the diagnostic process, their feedback must be sought and valued. |
Workshops
View
SESSION 4.A
Building Programs of Feedback for Improving Clinical Reasoning
Presenter
Dr Andrew Olson and Associate Professor Stephen Priestley
Description
Feedback is critical for continuous improvement. Clinical reasoning, like any human endeavour, requires feedback to enhance performance.
Despite this, feedback on clinical reasoning can be sporadic and it is not systematically embedded in everyday clinical practice nor in medical education. In this session, we will workshop building programs of feedback for improving clinical reasoning both in clinical practice and in education.
Implementing a feedback program on clinical reasoning will move your healthcare organisation and your learners closer to the goal of achieving diagnostic excellence.
SESSION 4.B
Designing and Implementing a Diagnostic Excellence Program for your hospital or clinic
Presenters
Carmel Crock OAM and Dr Anjali Dhulia
Description
In this workshop you will have the opportunity to work on designing and planning the implementation of a Diagnostic Excellence Program suitable for your workplace.
Prior to the workshop you will be provided with materials including the CDC's Core Elements of Hospital Diagnostic Excellence.
There will be a focus on how you will create a Diagnostic excellence strategy and action plan based on the 5 action domains: ensuring effective teamwork, developing a reliable diagnostic process, engaging patients and family members, optimising cognitive performance, and creating robust learning systems.
Participants will have the opportunity to present their draft Diagnostic Excellence Programs and receive feedback and suggestions from the facilitators and other participants.
This workshop will give you a strong foundation in building a Diagnostic Excellence Program to take to your hospital leadership, patient advocates and colleagues in order to advance diagnostic safety in your workplace.
SESSION 4.C
Embracing the unknown: Communicating uncertainty to enhance diagnostic excellence
Presenters
Dr Mary Dahm, Jen Morris and Laura Chien
Description
Everyone involved in the diagnostic process—from doctors and nurses, radiologists and pathologists, to the patient and their support people —experiences uncertainty. How can the diagnostic team effectively communicate uncertainty to ensure diagnosis is safe and patient-centred? This interactive workshop, developed by experts and advocates in health communication and patient safety, challenges common assumptions about uncertainty communication and introduces participants to evidence-based communication strategies for navigating these complex conversations.
Through guided reflection and discussion, this session will explore uncertainty communication in the context of diagnostic excellence, framed around safety, patient-centredness, ethical and professional considerations. Participants will learn how transparent discussions about diagnostic uncertainty can enhance safety and trust, empower patients, and support diagnostic excellence from diverse perspectives and contexts.
Learning objectives
1. Be familiar with the importance of transparent communication about uncertainty in clinical care from patient safety, patient centred care, ethical and professional perspectives.
2. Recognise and reflect on own concerns and assumptions about communicating uncertainty to patients and colleagues
3. Recognise and discuss strategies for communicating diagnostic uncertainty to patients and colleagues and their impact on diagnostic excellence.
Workshop facilitators
View
Symposium convenors
View
Program schedule
View
Time | Activity | |||
8:30am | Registration (Foyer Room G31) | |||
8:45am | Opening – Welcome (Room G31) | |||
9:00am | Session 1: International Keynotes (Room G31) | |||
9:00am - | Art and the Radical Act of Diagnosis Global Learning Objectives: Session Learning Objectives: Complexity and context in clinical reasoning | |||
10:30am | Morning tea (Sunken lounge) | |||
11:00am | Session 2: Local Keynotes (Room G31) | |||
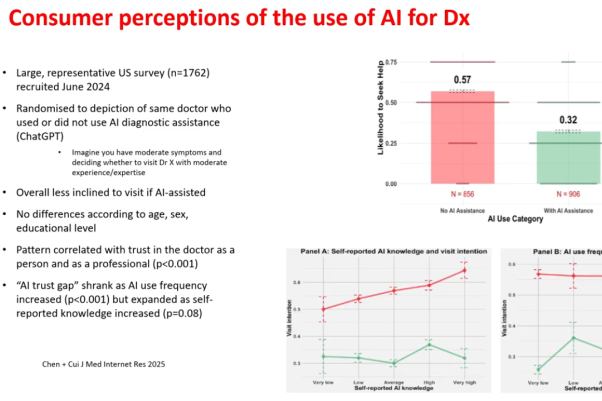
11:00am – 12:00pm | Penny for your thoughts: Improving how we think and diagnose at the bedside Introducing Diagnostic Excellence: Experience from a large Health Service How might AI assist in achieving diagnostic excellence? | |||
12:30pm | Lunch (Sunken lounge) | |||
1:30pm | Session 2 Continued: Local Keynotes (Room G31) | |||
1:30pm - 1:50pm | Improving Diagnosis: From Fallibility to Psychological Safety | |||
2:00pm | Session 3: Rapid Fire Oral presentations (Multiple Rooms) | |||
2:10pm | Session 3A | Session 3B | Session 3C | |
2:20pm | 3.A.2 Could it be HIV Increasing HIV Testing in Clinical Indicator Settings? Louise Owen | 3.B.2 Designing a Decision-Making Flowchart to Reduce Unnecessary CXR Ordering in the Emergency Department Joseph Miller | 3.C.2 The Relationship Between Patient or Caregiver Concern for Clinical Deterioration and Critical Illness in an Adult Population - A Retrospective Observational Cohort Study Simon Craig | |
2:30pm | 3.A.3 Exploration of in-hospital code stroke activation Lauren Sanders | 3.B.3 Developing Diagnostic Competencies for Nurse-led Pathways in the Emergency Department Deborah Digman | 3.C.3 How Creating a Safe Space for Patients Leads to Greater Diagnostic Accuracy Jennifer Neil | |
2:40pm | 3.A.4 The Outpatient Emergency Department Pathway to Cancer Diagnosis: Healthcare Engagement and Rural Treatment Disparities Caroline Thompson | 3.B.4 Investigation Framework Jane Birks | 3.C.4 Communicating Difficult Diagnoses in the Emergency Department. Gifar Hassan | |
2:50pm | 3.A.5 Absent Initial Clinical Impressions in ED: Time to Get Back to Basics Diana Egerton-Warburton | 3.B.5 Learning to Diagnose: Leveraging cognitive load theory (CLT) and metacognition to reduce diagnostic errors Pamela J. Ferrada | 3.C.5 Let‘s talk about HIV – Showcasing an Educational Partnership with People Living with HIV and Health Care Workers to Address Diagnostic Stigma Richard Keane | |
3:00pm | 3.C.6 Implementation of a structured clinical impression and management dotphrase in the electronic medical record as standard practice at Monash Health Emergency Departments: A stepped-wedge cluster-controlled analysis of the impact Diana Egerton-Warburton | 3.B.6 Evaluation of the Diagnostic Yield of CT and MR Modalities in Clinical Indications of Cranial Nerve Palsies Aaron Avenido | 3.C.6 The Art of Transforming Patient Feedback About Diagnostic Error into Diagnostic Excellence Carmel Crock | |
3:10pm | Afternoon Tea (Sunken lounge) | |||
3:30pm | Session 4: Concurrent workshops | |||
3:30pm - 4:30pm | Workshop 4A | Workshop 4B | Workshop 4C | |
4:35pm | Session 5: Plenary (Room G31) | |||
4:35pm - 4:55pm | Shaping the Future of Diagnosis: Symposium Wrap-up Facilitators: Julia Harrison & Carmel Crock | |||
5:00pm | Refreshments and networking (Sunken lounge) | |||
Contact us
If you have any questions about the symposium, please contact Emmelyn Vincent on emmelyn.vincent@monash.edu.
Upcoming symposium
For details about the next symposium, click here to visit the main symposium webpage.