ECCMID 2018
Supplementary materials for ECCMID 2018 abstract 989:
Modelling the benefit of echocardiography in patients with Staphylococcus aureus bacteraemia at low risk of endocarditis: implications for future trials.
GS Heriot1, SYC Tong2, AC Cheng1, D Liew1
1School of Public Health and Preventative Medicine, Monash University,
2The Peter Doherty Institute for Infection and Immunity, University of Melbourne
Supplementary methods
Model specification
The underlying model for the Monte Carlo simulation is designed to examine the survival benefit of echocardiography for a patient with Staphylococcus aureus bacteraemia (SAB) who does not have an intracardiac prosthetic device (prosthetic valve, pacemaker or implantable defibrillator), clinical signs of endocarditis, or another reason for prolonged antibiotic therapy, and is assessed as having a less than 5% probability of endocarditis by one of a number of scoring systems1.
The model is based on three disease states: uncomplicated SAB, clinically occult S. aureus left-sided native valve endocarditis (NVIE) without perivalvular complications (abscess), and NVIE with perivalvular abscess formation. Echocardiographic assessment has the same three possible results, with the correlation between the actual diseases state and the echocardiographic result being dependent on the diagnostic performance of each echocardiography strategy. Transthoracic echocardiography (TTE) and transoesophageal echocardiography (TOE) are not assumed to be independent tests given the similarities between the two procedures. The degree of statistical covariance between these tests is described as the percentage of the maximal covariance allowed by the observed diagnostic performance statistics2.
Treatment decisions are based on the results of echocardiography alone: patients thought not to have endocarditis receive two weeks of parenteral anti-staphylococcal therapy; those thought to have uncomplicated NVIE receive six weeks of parenteral anti-staphylococcal therapy; and those thought to have NVIE complicated by perivalvular abscess receive six weeks of parenteral anti-staphylococcal therapy and remedial cardiac surgery (assumed to be valve replacement). No other indications for surgery are considered in the model as, by definition, patients do not have clinical signs of endocarditis (including heart failure and systemic emboli).
The two strategies without echocardiography result in all patients receiving antibiotic therapy for the duration specified without surgery for perivalvular abscess.
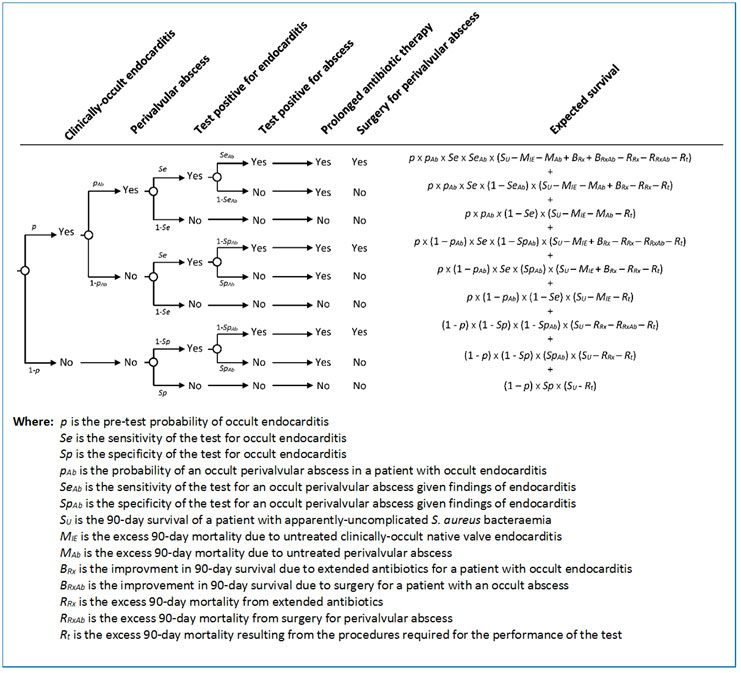
The outcome of the model is survival at 90 days. This outcome has been chosen to reflect the likely primary outcome of any future trial in this area to allow the model to inform statistical calculations. Survival outcomes in the model are additive. The expected survival resulting from any given strategy is the sum of the products of each possible permutation’s probability and its respective expected survival, as seen in the example decision tree presented in Figure 1.
Figure 1. Example decision tree and expected survival calculation used to model the outcome of each of the six echocardiography strategies.
Model inputs
Parameter estimates and error distributions were identified from the medical literature published to 16 November 2017 using a stepwise search strategy as outlined in a previous modelling paper3. These estimates are presented in Table 1.
Table 1. Parameter estimates, error distributions and sources.
Definition | Estimate | Range or 95% CI | Distribution | Sources |
Probability of disease | ||||
Prevalence of clinically-occult endocarditis in patients with apparently-uncomplicated S. aureus bacteraemia (SAB) and no intracardiac prosthetic device | Variable | 0-5% | 1,4 | |
Prevalence of perivalvular abscess among patients with clinically-occult native valve endocarditis (NVIE) | 15% | 10-20% | Triangular | 5-9 |
Probability of relapse if clinically-occult left-sided NVIE treated with two weeks of parenteral antibiotic therapy | 60% | 40-80% | Triangular | 10-18 |
Diagnostic performance of transoesophageal echocardiography (TOE) | ||||
Sensitivity of TOE for clinically-occult NVIE | 96% | 92-99% | Triangular | 19-23 |
Specificity of TOE for clinically-occult NVIE | 90% | 90-95% | Triangular | 19-23 |
Sensitivity of TOE for perivalvular abscess in patients with NVIE | 75% | 40-90% | Triangular | 7,9,24-26 |
Specificity of TOE for perivalvular abscess in patients with NVIE | 98% | 96-100% | Triangular | 7,9,24-26 |
Diagnostic performance of transthoracic echocardiography (TTE) | ||||
Apparent sensitivity of TTE for occult NVIE (as compared to TOE) | 58% | 53-62% | Beta | 27 |
Apparent specificity of TTE for occult NVIE | 92% | 91-93% | Beta | 17,18,27 |
Apparent sensitivity of TTE for perivalvular abscess | 48% | 29-67% | Beta | 27 |
Apparent specificity of TTE for perivalvular abscess in occult NVIE | 100% | 99-100% | Beta | 27 |
%maximum statistical covariance between TTE and TOE | 25% | 0-50% | Triangular | No data |
Survival estimates for various diseases states | ||||
90-day survival of patients with apparently uncomplicated SAB | 80% | 76-83% | Beta | 28 |
Excess mortality associated with diagnosed and treated NVIE | 15% | 10-25% | Triangular | 29-31 |
Additional mortality associated with relapsed partially-treated NIVE | 15% | 12-17% | Triangular | 32,33 |
Excess mortality associated with diagnosed and treated perivalvular abscess in NVIE | 15% | 0-30% | Triangular | 5,7,34-36 |
Additional mortality if perivalvular abscess initially goes unrecognised | 15% | 0-30% | Triangular | 5,7,34-36 |
Risks associated with testing and treatment | ||||
Excess mortality due to the procedures required for TOE | Variable | 0.01-1% | 37-40 | |
Excess mortality due to the procedures required for TTE | 0% | Assumed | ||
Excess mortality due to adverse drug events in weeks 2-6 of therapy | 0.2% | 0-0.7% | Beta | 41,42 |
Excess mortality due to line infection arising in weeks 2-6 of therapy | 0.3% | 0.1-0.8% | Beta | 43-54 |
Excess mortality due to cardiac surgery for perivalvular abscess | 5% | 3-9% | Triangular | 55,56 |
Multiple independent sources in general agreement with each other were found for each of these parameters, with three exceptions:
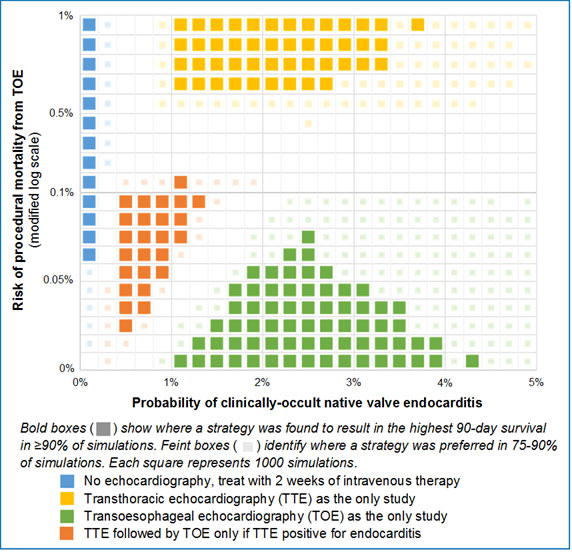
- As extensively discussed in a previous paper3, estimates for the procedure-related mortality of TOE vary from 0.01% to 1% depending on study methodology. This discrepancy is unresolvable with the currently available literature. As a result, we have chosen to report our results primarily as a two-way sensitivity (strategy) analysis, using the probability of endocarditis and the mortality of TOE as the variables.
- The likelihood of relapse if unrecognised clinically-occult S. aureus NVIE is treated with only two weeks of parenteral anti-staphylococcal therapy is essentially unknown. There are no studies examining the deliberate use of short-course therapy for left-sided endocarditis, and the available studies reporting relapses of endocarditis after the inadvertent use of abbreviated therapy do not provide a reliable denominator to assess how often this may occur.
The estimate we have used for our analysis comes from dividing the relapse rate among unselected patients with central line-associated SAB treated with two weeks of antibiotic therapy (6%12) by the prevalence of endocarditis among such patients in series with high rates of TOE (10-15%14-16).
In addition, we have assessed the impact of the traditional estimate for this parameter (100%13) in the sensitivity analyses presented below.
- The maximal statistical covariance (or non-independence) of TTE and TOE is also unknown, as there are no studies rigorously comparing the distribution of the results of both modalities against an independent reference standard (e.g. autopsy or surgical findings). Previous modelling studies57 have assumed these tests to be independent, but the similarities in technology (ultrasound) and target abnormalities (structural abnormalities of cardiac valves and associated structures) ensure some degree of correlation in their errors.
We have chosen to model a low but non-zero degree of non-independence between TTE and TOE (~25% the maximum possible statistical covariance) in our primary results, and a higher degree (~75%) in the sensitivity analysis presented below. The effect of these degrees of non-independence on the true diagnostic performance of TTE for NVIE can be seen in Table 2.
Table 2. Effect of non-independence of TTE and TOE on the true diagnostic performance of TTE for left-sided native valve endocarditis.
Sensitivity | Specificity | |
Performance of TOE for NVIE compared to pathological findings19 | 96% | 90% |
Apparent performance of TTE compared to TOE in series with 18% prevalence of NVIE27 | 58% | 92% |
True performance of TTE assuming: | ||
Statistical independence of TTE and TOE | 60% | 93% |
25% maximal statistical covariance | 54% | 90% |
50% maximal statistical covariance | 48% | 88% |
75% maximal statistical covariance | 42% | 85% |
100% maximal statistical covariance | 37% | 83% |
Sensitivity analyses
The effect of universal relapse of NVIE after short-course therapy
As described above, we estimated the proportion of cases of clinically-occult NVIE that would relapse after inadvertent receipt of two weeks of parenteral antibiotic therapy to be 60% (range 40-80%). Figure 2 shows the effect of assuming that all such patients would suffer relapses. The increased mortality associated with under-treatment of NVIE that results from this assumption causes a linear transformation in the horizontal axis compared to our base-case scenario.
Figure 2. Preferred echocardiography strategy assuming 100% relapse rate for NVIE after inadvertent short-course treatment.
The effect of high statistical covariance between TTE and TOE
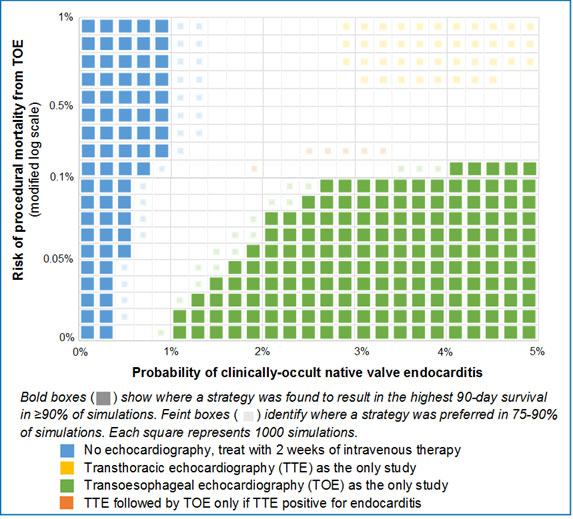
As the degree of non-independence of TTE and TOE increases, the informational value of strategies employing two studies falls. Figure 3 shows the effect of assuming a high degree of correlation between the errors of TTE and TOE (75% maximal possible statistical covariance). TTE as the initial test followed by TOE if the TTE is positive no longer appears as a preferred strategy.
Figure 3. Preferred echocardiography strategy assuming a high degree of statistical covariance between TTE and TOE.
References
- Heriot GS, Cronin K, Tong SY, Cheng AC, Liew D. Criteria for identifying patients with Staphylococcus aureus bacteremia who are at low risk of endocarditis: a systematic review. Open Forum Infect Dis. 2017;4(4):ofx261.
- Vacek PM. The effect of conditional dependence on the evaluation of diagnostic tests. Biometrics. 1985;41(4):959-968.
- Heriot GS, Tong SY, Cheng AC, Liew D. What risk of endocarditis is low enough to justify the omission of transoesophageal echocardiography in Staphylococcus aureus bacteraemia? A narrative review. Clinical Microbiology and Infection. 2018.
- Bai AD, Agarwal A, Steinberg M, et al. Clinical predictors and clinical prediction rules to estimate initial patient risk for infective endocarditis in Staphylococcus aureus bacteraemia: a systematic review and meta-analysis. Clin Microbiol Infect. 2017;23(12):900-906.
- Anguera I, Miro JM, Cabell CH, et al. Clinical characteristics and outcome of aortic endocarditis with periannular abscess in the International Collaboration on Endocarditis Merged Database. Am J Cardiol. 2005;96(7):976-981.
- Anguera I, Miro JM, Evangelista A, et al. Periannular complications in infective endocarditis involving native aortic valves. Am J Cardiol. 2006;98(9):1254-1260.
- Choussat R, Thomas D, Isnard R, et al. Perivalvular abscesses associated with endocarditis; clinical features and prognostic factors of overall survival in a series of 233 cases. Perivalvular Abscesses French Multicentre Study. Eur Heart J. 1999;20(3):232-241.
- Arnett EN, Roberts WC. Valve ring abscess in active infective endocarditis. Frequency, location, and clues to clinical diagnosis from the study of 95 necropsy patients. Circulation. 1976;54(1):140-145.
- Hill EE, Herijgers P, Claus P, Vanderschueren S, Peetermans WE, Herregods MC. Abscess in infective endocarditis: the value of transesophageal echocardiography and outcome: a 5-year study. Am Heart J. 2007;154(5):923-928.
- Mansur AJ, Dal Bó CM, Fukushima JT, Issa VS, Grinberg M, Pomerantzeff PM. Relapses, recurrences, valve replacements, and mortality during the long-term follow-up after infective endocarditis. Am Heart J. 2001;141(1):78-86.
- Fernández-Hidalgo N, Almirante B, Tornos P, et al. Immediate and long-term outcome of left-sided infective endocarditis. A 12-year prospective study from a contemporary cohort in a referral hospital. Clin Microbiol Infect. 2012;18(12):E522-530.
- Jernigan JA, Farr BM. Short-course therapy of catheter-related Staphylococcus aureus bacteremia: a meta-analysis. Ann Intern Med. 1993;119(4):304-311.
- Rosen AB, Fowler VG, Jr., Corey GR, et al. Cost-effectiveness of transesophageal echocardiography to determine the duration of therapy for intravascular catheter-associated Staphylococcus aureus bacteremia. Ann Intern Med. 1999;130(10):810-820.
- Fowler VG, Jr., Justice A, Moore C, et al. Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin Infect Dis. 2005;40(5):695-703.
- Joseph JP, Meddows TR, Webster DP, et al. Prioritizing echocardiography in Staphylococcus aureus bacteraemia. J Antimicrob Chemother. 2013;68(2):444-449.
- Engemann JJ, Friedman JY, Reed SD, et al. Clinical outcomes and costs due to Staphylococcus aureus bacteremia among patients receiving long-term hemodialysis. Infect Control Hosp Epidemiol. 2005;26(6):534-539.
- Khatib R, Sharma M. Echocardiography is dispensable in uncomplicated Staphylococcus aureus bacteremia. Medicine (Baltimore). 2013;92(3):182-188.
- Rasmussen RV, Host U, Arpi M, et al. Prevalence of infective endocarditis in patients with Staphylococcus aureus bacteraemia: the value of screening with echocardiography. Eur J Echocardiogr. 2011;12(6):414-420.
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-3128.
- Shapiro SM, Young E, De Guzman S, et al. Transesophageal echocardiography in diagnosis of infective endocarditis. Chest. 1994;105(2):377-382.
- Erbel R, Rohmann S, Drexler M, et al. Improved diagnostic value of echocardiography in patients with infective endocarditis by transoesophageal approach. A prospective study. Eur Heart J. 1988;9(1):43-53.
- Shively BK, Gurule FT, Roldan CA, Leggett JH, Schiller NB. Diagnostic value of transesophageal compared with transthoracic echocardiography in infective endocarditis. J Am Coll Cardiol. 1991;18(2):391-397.
- Mügge A, Daniel WG, Frank G, Lichtlen PR. Echocardiography in infective endocarditis: reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J Am Coll Cardiol. 1989;14(3):631-638.
- Daniel WG, Mügge A, Martin RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med. 1991;324(12):795-800.
- Cicioni C, Di Luzio V, Di Emidio L, et al. Limitations and discrepancies of transthoracic and transoesophageal echocardiography compared with surgical findings in patients submitted to surgery for complications of infective endocarditis. J Cardiovasc Med (Hagerstown). 2006;7(9):660-666.
- Koo HJ, Yang DH, Kang JW, et al. Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography: comparison with intra-operative findings. Eur Heart J Cardiovasc Imaging. 2017.
- Bai AD, Steinberg M, Showler A, et al. Diagnostic Accuracy of Transthoracic Echocardiography for Infective Endocarditis Findings Using Transesophageal Echocardiography as the Reference Standard: A Meta-Analysis. J Am Soc Echocardiogr. 2017;30(7):639-646.
- Su CH, Chang SC, Yan JJ, Tseng SH, Chien LJ, Fang CT. Excess mortality and long-term disability from healthcare-associated staphylococcus aureus infections: a population-based matched cohort study. PLoS One. 2013;8(8):e71055.
- Brown J, Brown K, Forrest A. Vancomycin AUC24/MIC ratio in patients with complicated bacteremia and infective endocarditis due to methicillin-resistant Staphylococcus aureus and its association with attributable mortality during hospitalization. Antimicrob Agents Chemother. 2012;56(2):634-638.
- Le Moing V, Alla F, Doco-Lecompte T, et al. Staphylococcus aureus Bloodstream Infection and Endocarditis--A Prospective Cohort Study. PLoS One. 2015;10(5):e0127385.
- Kaasch AJ, Barlow G, Edgeworth JD, et al. Staphylococcus aureus bloodstream infection: a pooled analysis of five prospective, observational studies. J Infect. 2014;68(3):242-251.
- Albertson J, McDanel JS, Carnahan R, et al. Determination of risk factors for recurrent methicillin-resistant Staphylococcus aureus bacteremia in a Veterans Affairs healthcare system population. Infect Control Hosp Epidemiol. 2015;36(5):543-549.
- Chu VH, Sexton DJ, Cabell CH, et al. Repeat infective endocarditis: differentiating relapse from reinfection. Clin Infect Dis. 2005;41(3):406-409.
- Chan KL. Early clinical course and long-term outcome of patients with infective endocarditis complicated by perivalvular abscess. CMAJ. 2002;167(1):19-24.
- Lerakis S, Robert Taylor W, Lynch M, et al. The role of transesophageal echocardiography in the diagnosis and management of patients with aortic perivalvular abscesses. Am J Med Sci. 2001;321(2):152-155.
- Vikram HR, Buenconsejo J, Hasbun R, Quagliarello VJ. Impact of valve surgery on 6-month mortality in adults with complicated, left-sided native valve endocarditis: a propensity analysis. Jama. 2003;290(24):3207-3214.
- Daniel WG, Erbel R, Kasper W, et al. Safety of transesophageal echocardiography. A multicenter survey of 10,419 examinations. Circulation. 1991;83(3):817-821.
- Khandheria BK, Seward JB, Bailey K, et al. Safety of transesophageal echocardiography: experience with 2070 consecutive procedures. Journal of the American College of Cardiology. 1991;17(2):A20.
- Min JK, Spencer KT, Furlong KT, et al. Clinical features of complications from transesophageal echocardiography: a single-center case series of 10,000 consecutive examinations. J Am Soc Echocardiogr. 2005;18(9):925-929.
- Klein AL, Grimm RA, Murray RD, et al. Use of transesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. N Engl J Med. 2001;344(19):1411-1420.
- Blumenthal KG, Youngster I, Rabideau DJ, et al. Peripheral blood eosinophilia and hypersensitivity reactions among patients receiving outpatient parenteral antibiotics. J Allergy Clin Immunol. 2015;136(5):1288-1294.e1281.
- Barr DA, Semple L, Seaton RA. Outpatient parenteral antimicrobial therapy (OPAT) in a teaching hospital-based practice: a retrospective cohort study describing experience and evolution over 10 years. Int J Antimicrob Agents. 2012;39(5):407-413.
- Htin AK, Friedman ND, Hughes A, et al. Outpatient parenteral antimicrobial therapy is safe and effective for the treatment of infective endocarditis: a retrospective cohort study. Intern Med J. 2013;43(6):700-705.
- Larioza J, Heung L, Girard A, Brown RB. Management of infective endocarditis in outpatients: clinical experience with outpatient parenteral antibiotic therapy. South Med J. 2009;102(6):575-579.
- Cervera C, del Rio A, Garcia L, et al. Efficacy and safety of outpatient parenteral antibiotic therapy for infective endocarditis: a ten-year prospective study. Enferm Infecc Microbiol Clin. 2011;29(8):587-592.
- Cervera C, del Rio A, Garcia L, et al. Efficacy and safety of outpatient parenteral antibiotic therapy for infective endocarditis: a ten-year prospective study. Enferm Infecc Microbiol Clin. 2011;29(8):587-592.
- Amodeo MR, Clulow T, Lainchbury J, et al. Outpatient intravenous treatment for infective endocarditis: safety, effectiveness and one-year outcomes. J Infect. 2009;59(6):387-393.
- Tokars JI, Cookson ST, McArthur MA, Boyer CL, McGeer AJ, Jarvis WR. Prospective evaluation of risk factors for bloodstream infection in patients receiving home infusion therapy. Ann Intern Med. 1999;131(5):340-347.
- Baharoon S, Almodaimeg H, Al Watban H, et al. Home intravenous antibiotics in a tertiary care hospital in Saudi Arabia. Ann Saudi Med. 2011;31(5):457-461.
- Kieran J, O'Reilly A, Parker J, Clarke S, Bergin C. Self-administered outpatient parenteral antimicrobial therapy: a report of three years experience in the Irish healthcare setting. Eur J Clin Microbiol Infect Dis. 2009;28(11):1369-1374.
- Upton A, Ellis-Pegler RB, Woodhouse A. Outpatient Parenteral Antimicrobial Therapy (OPAT): a review of experience at Auckland Hospital. N Z Med J. 2004;117(1200):U1020.
- Ziegler MJ, Pellegrini DC, Safdar N. Attributable mortality of central line associated bloodstream infection: systematic review and meta-analysis. Infection. 2015;43(1):29-36.
- Tedja R, Gordon SM, Fatica C, Fraser TG. The descriptive epidemiology of central line-associated bloodstream infection among patients in non-intensive care unit settings. Infect Control Hosp Epidemiol. 2014;35(2):164-168.
- Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol. 2014;25(12):2927-2941.
- Martínez-Sellés M, Muñoz P, Arnáiz A, et al. Valve surgery in active infective endocarditis: a simple score to predict in-hospital prognosis. Int J Cardiol. 2014;175(1):133-137.
- David TE, Gavra G, Feindel CM, Regesta T, Armstrong S, Maganti MD. Surgical treatment of active infective endocarditis: a continued challenge. J Thorac Cardiovasc Surg. 2007;133(1):144-149.
- Heidenreich PA, Masoudi FA, Maini B, et al. Echocardiography in patients with suspected endocarditis: a cost-effectiveness analysis. Am J Med. 1999;107(3):198-208.
COPYRIGHT © 2018 THE AUTHORS