Pancreatic cancer (PDAC) is one of the most lethal types of human cancer due to its aggressive nature and lack of effective treatments. Obesity further increases cancer risk by altering the metabolism of cancer cells. Sadly, enormous efforts in treatment development have not yet improved the survival rate nor the off-target effects. New therapeutic targets and treatments are critically needed.
>70% of pancreatic cancers originate from the head of the pancreas, where the pancreas is connected to both the gut and adipose tissue. However, the factors that promote cancer formation in this area are unknown, and no clinically relevant model recapitulates this key pathological feature of PDAC.
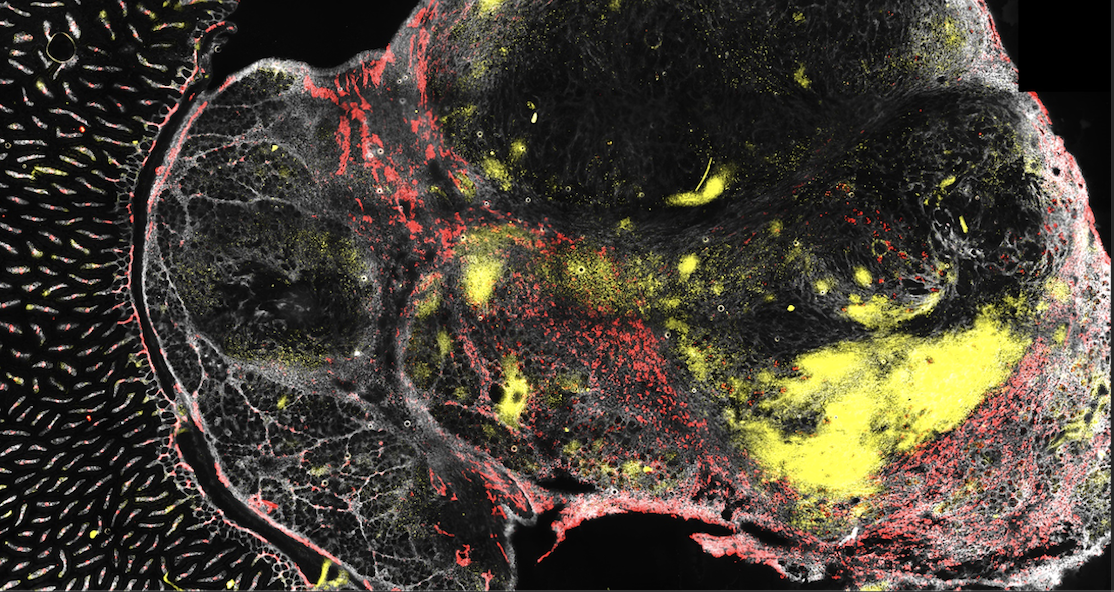
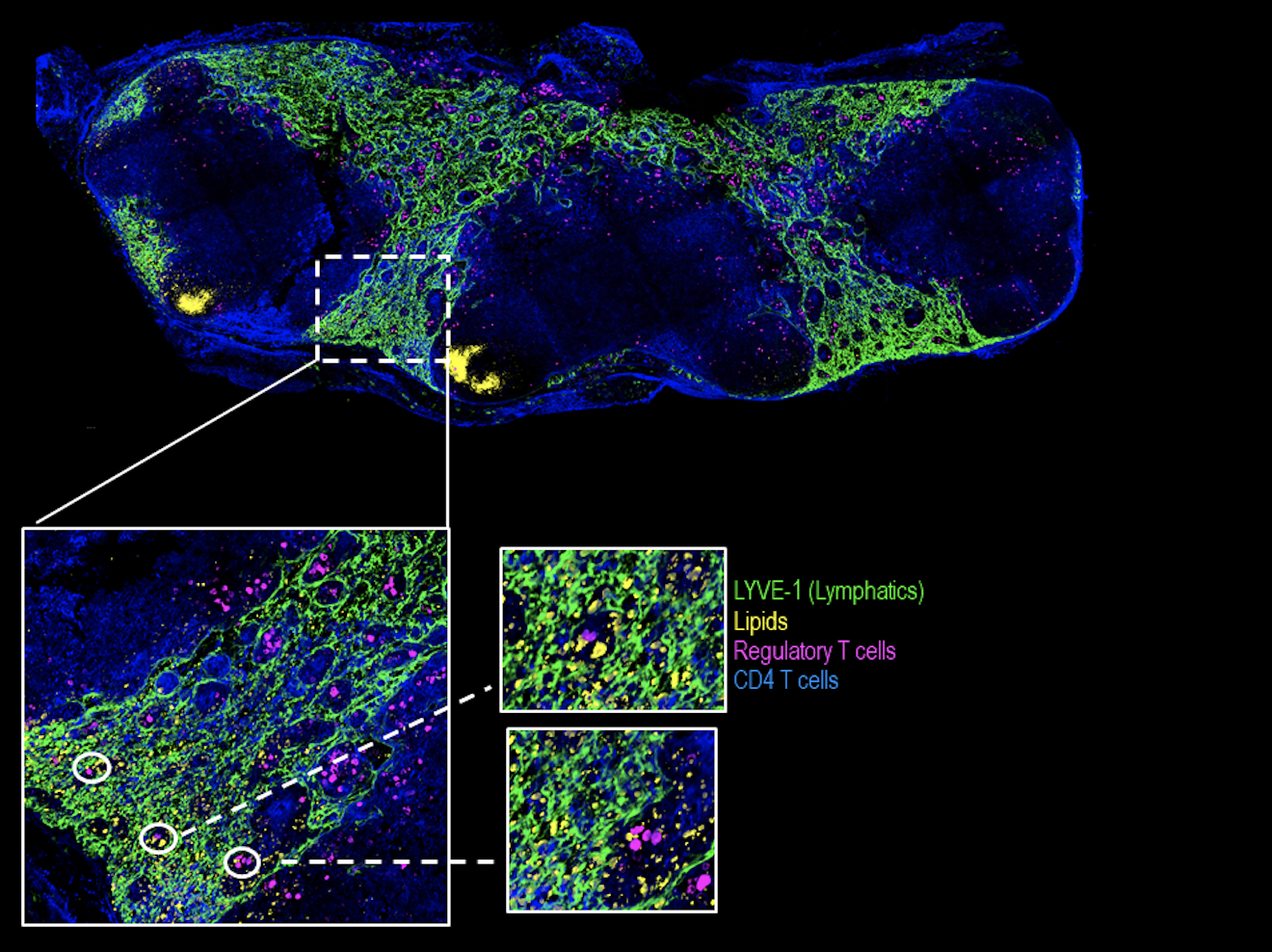
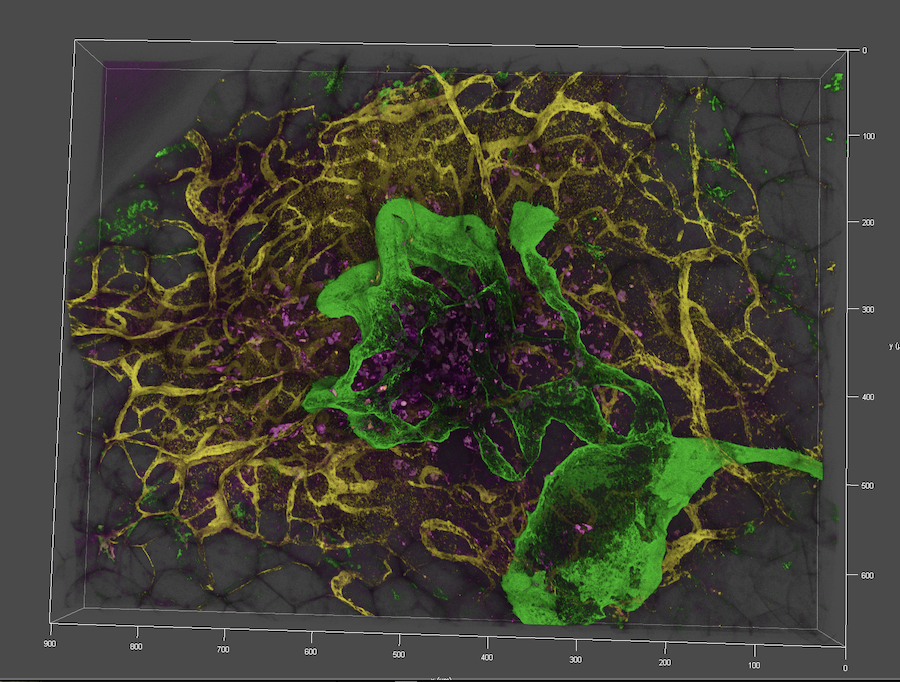
Our data reveal a previously undescribed crosstalk between the gut-draining lymphatics and pancreas where, especially in obesity, lymphatics supplies energy source in the form of dietary lipids to the pancreas which modifies cancer cell metabolism and promotes metastasis.
We will:
1. Establish the first clinically relevant, PDAC model at the head of the pancreas to investigate the cause of cancer formation.
2. Examine how ‘obesity-associated lipids’ modify cancer metabolism and promote PDAC.
3. Stop PDAC by shutting done the lymphatic ‘energy supply’ via targeting lymph-pancreas interactions with minimal off-target effects.
Crohn's disease (CD) and ulcerative colitis (UC) are inflammatory bowel diseases (IBD) that are characterised by chronic and aberrant mucosal immune response. Factors including genetic susceptibility, environmental factors, dysregulation in gut immune cells and microbiota have been shown to contribute to IBD progression. Recent studies also suggest the involvement of vascular dysfunction in IBD. While the pathogenic role of blood vessel proliferation is well defined, the changes in lymphatic function in IBD are less understood.
Despite the improvements in diagnostic modalities and treatments for IBD, a substantial proportion of patients are either at the refractory phase of the available treatments or develop colitis-associated cancer. New therapeutic targets of IBD are thus necessary to manage the disease more adequately.
The project aims to:
1. Investigate the changes in lymphatic function and the associated immune mechanisms in IBD
2. Investigate how normalise lymphatic function contribute to mucosal healing
3. Explore lymphatic therapeutic targets to treat IBD
Type 2 diabetes (T2D) exacerbates cardiovascular diseases, including atherosclerosis. Atherosclerosis is the major cause of heart infarction, leading to ~1/3rd of global and ~27% of Australian mortality. Current therapies focus on lipid-lowering but have sub-optimal efficacy. There is an urgent need to identify novel mechanisms and therapeutic targets to improve treatment. Adipose tissue inflammation promotes T2D and atherosclerosis. Aberrant T and B cells in tertiary lymphoid tissues (TLO) drive adipose tissue inflammation. TLOs form part of the mesenteric lymphatics, act as immune sentinels to recruit large numbers of inflammatory cells and support rapid immune responses in infection.
We aim to investigate:
1: To dissect the crosstalk between TLO lymphatics and immune cells in obesity and insulin resistance.
2: To establish TLO-specific immune interventions that reverse obesity and insulin resistance