Monash research targets the multilayered causes of adult eczema resistant to new antibody therapy
For many adults living with severe atopic dermatitis, or eczema, the drug Dupilumab has been a resounding success. But as is common in complex conditions, even a proclaimed miracle drug falls short for some users. The quest to find out why is highlighting how little we know about the skin microbiome, let alone its interactions with the immune system and our genetic makeup.
Atopic dermatitis affects 10 to 20 per cent of children. Many grow out of it, but prevalence in adulthood in Australia is 5% and disease is usually severe and disruptive, with flare-ups causing insomnia, itchiness, pain and psychological distress.
The asthma link
About a quarter of people with eczema also have asthma. The risk appears to increase in people who have severe eczema, with suspicions centring on elevated immunoglobulin levels, genetics, and environmental triggers.
Scientist Celine Pattaroni knows this well, having come to the skin via research on asthma in early childhood. She’s leading a multidisciplinary team that’s been awarded a $1.4m Pathways grant by pharmaceutical giant Sanofi to explore the drivers of severe AD on a range of levels, and how these affect Dupilumab’s efficacy.
“Some patients don’t respond well, or develop rare side effects, such as facial redness or conjunctivitis,” Pattaroni explains. “So one part of the project is to try to understand why some patients respond well to the drug and some don’t.”
A special drug class
It’s just three years since Dupilumab, the first monoclonal antibody (maB) drug for AD, was listed on the Australian Pharmaceutical Benefits Scheme (PBS) for people living with severe forms of eczema and/or asthma. It blocks the signalling of two proteins known to cause inflammation, and in most patients has significantly reduced itching and other symptoms. The treatment is usually lifelong injections every two to four weeks.
The therapeutic pipeline for AD reflects the different systems being targeted in clinical trials: these drugs include bacterial strains targeting the microbiome, and biologics variously targeting the adaptive immune response, the innate immune response and itching.
It’s a class of drugs on the rise: another maB, Lebrikizumab, manufactured by Eli Lilly, has just been listed by Australia’s Therapeutic Goods Administration. In just eight years, the number of internationally approved maBs has shot from 30 to around 130, a more than four-fold increase representing a global market of US$221 million.
They represent a step change from the treatments that were standard for decades — creams, ointments and tablets, often ineffective, and containing steroids with brutal side effects.
“This class of drug is very special,” Pattaroni says. “Because it's an antibody, it is very specific in targeting the proteins that cause inflammation. And although we know what it does to the main immune cells, no one has looked at what it does on other cell types, such as structural skin cells or cells from the nervous system.”
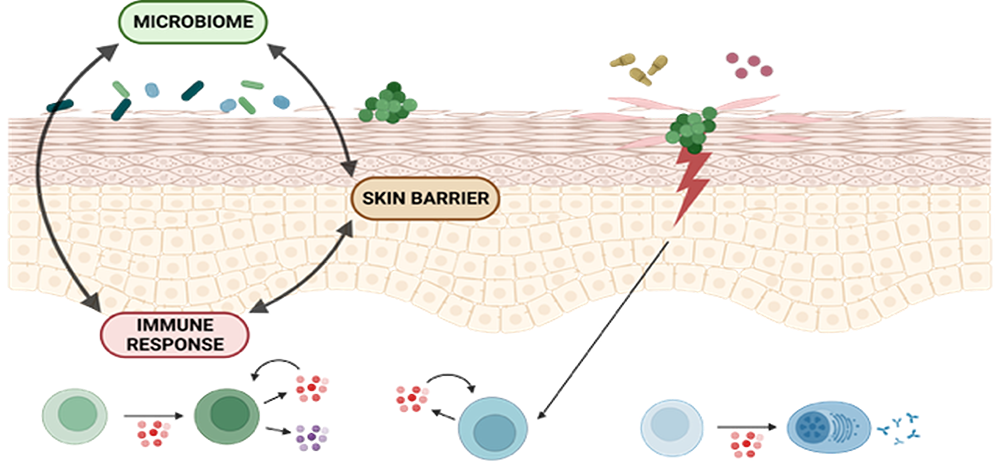
Image supplied by C Pattaroni .
Multiomics: “crosstalk” between systems
Pattaroni is using her expertise in both immunology and bioinformatics to mine vast amounts of data from clinical samples to map the “crosstalk” between structural skin cells, the immune system and microbes - a “multiscale” landscape - and their response to treatment.
“If we look at multiple layers, we will get more in-depth and holistic information about what is happening in the skin.
“We used to think that only immune cells were sensitive to immune cues. But more and more, we see that skin cells sense all these immune cues more than we thought.”
Known as multiomics, this multilayered approach is a relative newcomer to dermatological research, and an as yet uncommon feature of grants like this. It comprises genomics (DNA); transcriptomics and proteomics (RNA and the instructions and proteins it produces); and metabolomics (chemical cues or signals caused by metabolites). It’s more an Escher print than a layer cake, offering different dimensions and vantage points, and unexpected connections. The end game is to pinpoint something - a metabolite or other biomarker that could predict drug response.
Staph and the skin microbiome
Pattaroni expects multiomics to uncover the impact of a disrupted skin microbiome in people with AD. “We’ve known for a long time that many patients have an increase of staphylococcus bacteria on their eczema lesions. It takes over and crowds out the healthy bugs.
“Fungi is a lesser known part of the skin microbiome,” she adds. “We're starting to see a lot of studies in the gut and in the lungs, pointing towards the idea that that might play a role as well.”
The project also includes immunologist and fellow asthma expert Professor Ben Marsland and dermatologist Professor Johannes Kern. It is part of the new SkIIN Discovery Program, part of the School of Translational Medicine, in partnership with the Monash School of Public Health and Preventive Medicine, located in the Alfred Research Alliance.It will lead innovative dermatology research and clinical trials spanning common skin conditions through to skin cancers.
“We think this is a big win for interdepartmental collaborations and the translational research approach at Monash and Alfred Health,” says Kern. “I’m very excited that this is firing the starting gun on translational research work on a very common and impactful skin disease.”