Professor Arvind Sehgal Leads International Team in Advancing Precision Medicine for Critically Ill Newborns
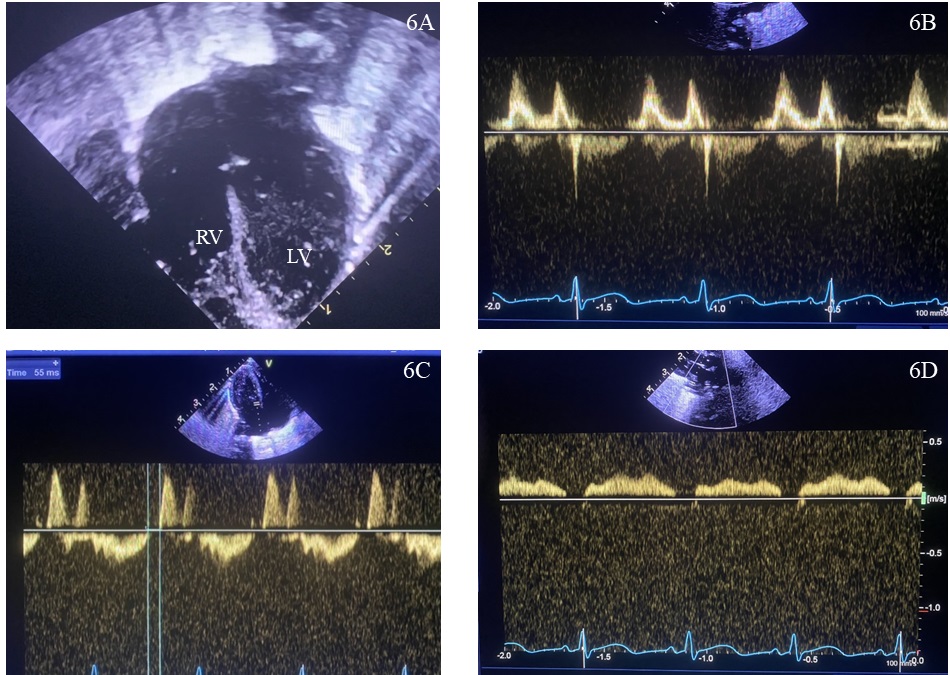
Example images obtained from different forms of echocardiographic analysis
An international team led by Professor Arvind Sehgal has called for a shift in how clinicians treat the most fragile babies in neonatal intensive care. In a new review, published in the Journal of Perinatology, the authors argue that current “one-size-fits-all” treatment protocols may be doing more harm than good—and propose a more personalised, physiology-driven approach to caring for critically ill newborns.
Professor Sehgal, who leads cardiovascular research at Monash Children's Hospital and the School of Clinical Sciences at Monash Health, co-authored the paper with collaborators Dr Matthew Buckingham, Dr Rachael Hyland, and Professor Patrick McNamara from Australia, New Zealand, and the United States. Together, they examined clinical data and case studies from three high-risk groups: infants of diabetic mothers, twins affected by twin-to-twin transfusion syndrome, and preterm babies with severe lung disease. While these babies often present with similar symptoms, such as breathing difficulties or low oxygen levels, the review shows that the underlying heart and blood vessel problems are markedly different, and so are the treatments they require.
At the heart of the review is a call for the mandatory use of Neonatologist Performed Echocardiography (NPE) in these high-risk groups. NPE is a specialised bedside heart ultrasound that provides real-time insight into how a newborn’s heart is functioning: blood flow, pressure, and cardiac output. This allows clinicians to go beyond assumptions and tailor treatment decisions to each baby’s unique cardiovascular profile.
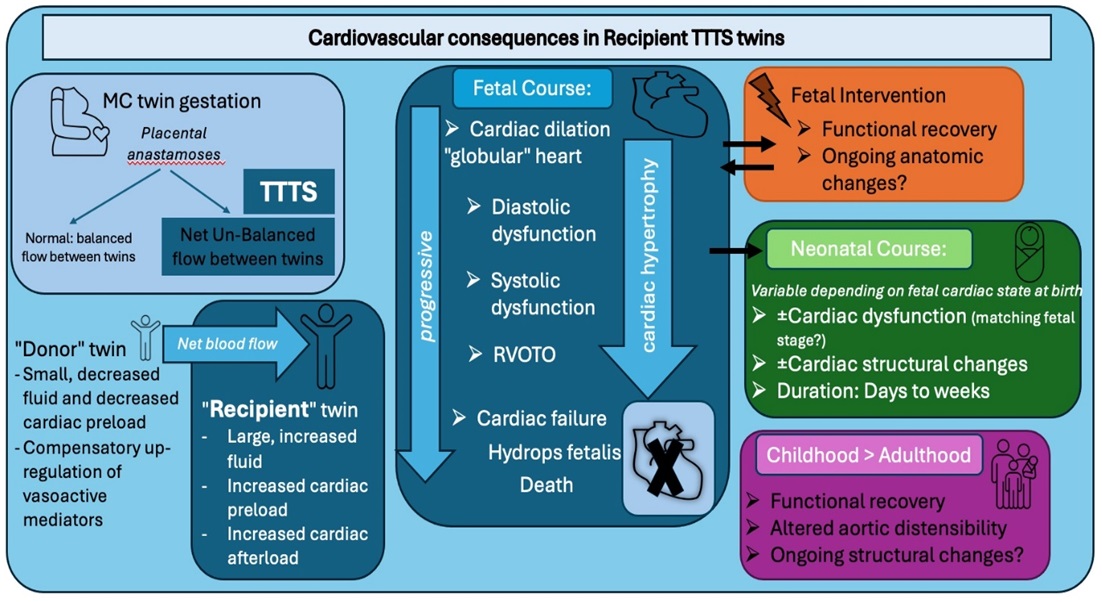
Flowchart describing the cardiovascular consequences in twin-to-twin transfusion syndrome recipient twins. TTTS: twin-to-twin transfusion syndrome, MC: monochorionic, RVOTO: right ventricular outflow tract obstruction
The review highlights how babies with different conditions can face very different heart challenges, even when their symptoms look similar. For example, babies born to mothers with diabetes may develop thickened heart muscle that blocks blood flow. Twins affected by twin-to-twin transfusion syndrome often have dangerously imbalanced blood volumes, putting strain on their hearts. And in some premature babies with severe lung disease, the real issue may be high blood pressure or poor heart function, factors that are often missed.
Historically, treatments in neonatal intensive care have focused on supporting the lungs, because breathing difficulties are usually the most obvious and urgent signs of distress. But this lung-first approach can overlook underlying heart problems that may be driving or worsening the baby's condition. The authors argue that by using NPE to assess each baby’s cardiovascular function in detail, clinicians can better understand what’s really going wrong—and choose treatments that are safer and more effective.
The paper also challenges conventional thinking by showing that some babies may benefit from medications typically used to treat high blood pressure in adults - such as ACE inhibitors - rather than standard respiratory support or pulmonary vasodilators. In doing so, it makes a compelling case for replacing rigid treatment protocols with precision medicine that responds to each baby’s specific needs.
Professor Sehgal explains that this approach represents "the hallmark of precision in clinical decision-making." Rather than applying the same treatment protocol to every baby with similar symptoms, doctors can tailor their approach based on what's actually causing each baby's specific problems.
This work highlights how international collaboration can advance medical care in neonatal intensive care units. By moving towards more precise, individualised treatments, Professor Sehgal and his colleagues hope their findings will prompt greater uptake of targeted cardiovascular assessments in NICUs worldwide, ultimately improving survival and long-term health outcomes for some of the most vulnerable patients in medicine, giving these tiny patients the best possible start in life.
About Monash University
Monash University is Australia’s largest university with more than 80,000 students. In the 60 years since its foundation, it has developed a reputation for world-leading high-impact research, quality teaching, and inspiring innovation.
With four campuses in Australia and a presence in Malaysia, China, India, Indonesia and Italy, it is one of the most internationalised Australian universities.
As a leading international medical research university with the largest medical faculty in Australia and integration with leading Australian teaching hospitals, we consistently rank in the top 50 universities worldwide for clinical, pre-clinical and health sciences.
For more news, visit Medicine, Nursing and Health Sciences or Monash University.
MEDIA ENQUIRIES